-
Presents w/ academic/behavioral problems + inattn/hyperactivity/impulsivity sx, 4-18 yo
Eval per DSM-5,1 incl documentation of sx/impairment in ≥2 major settings (ie, social, academic, occupational) and r/o alternative cause [B/S]; obtain info from child or adolescent,2 parents,3 and school4 Screen for comorbid conditions [B/S]: Emotional/behavioral,5 developmental,6 or physical7 - If newly diagnosed ADHD in adolescent (age 12 to 18 yo): at minimum, assess s/sx of substance abuse, anxiety, depression, and learning disabilities
- Treat any comorbid disorders if w/in clinician’s expertise; evaluate further or refer to appropriate subspecialist for dx and tx as needed; [C/R]
- Address urgent conditions8 immediately w/ services capable of handling crisis situations
- Provide education to family and child
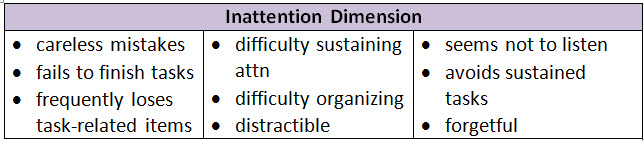
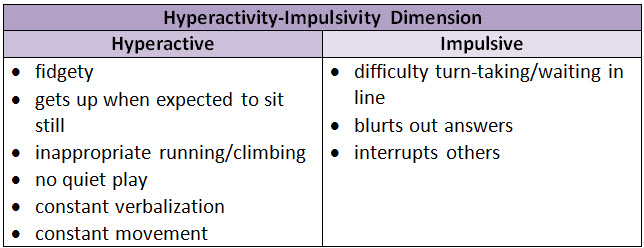
Inattention-predominant ADHD: ≥69 of 9 for ≥6 mo (and <6 hyperactive/impulsive sx)10 Hyperactive/impulsive-predominant: ≥69 of 9 for ≥6 mo (and <6 inattention sx)10 Combination type: ≥69 of 9 from both inattention and hyperactivity-impulsivity dimensions for ≥6 mo Apply DSM-5 criteria - Some behaviors must be present before age 1210
- Behaviors must show presence of sx affecting 2 or more settings (eg, home, school, or work; w/ friends or relatives; in other activities) [B/S]
- Ensure obvious signs of social/school/work dysfxn
- Sx must be separate from schizophrenia or another psychotic disorder and not explained by another mental health dx (ie, mood/anxiety/dissociative/personality disorders, substance intoxication or withdrawal) [B/S]
If sx arise suddenly, w/o any previous hx, consider other conditions incl: mood or anxiety disorders, substance use, head trauma, physical/sexual abuse, neurodegenerative disorders, sleep disorders (incl sleep apnea) or major family/school stress (eg, bullying) In adolescent/young adult pts: Consider potential for false reporting/misrepresentation of sx to obtain meds for other than appropriate medicinal use (ie, diversion, secondary gain) Footnotes 1 DSM-5 criteria define 4 dimensions of ADHD:
• attention-deficit/hyperactivity disorder primarily of the inattentive presentation (ADHD/I) (314.00 - F90.0);
• attention-deficit/hyperactivity disorder primarily of the hyperactive-impulse presentation (ADHD/HI) (314.01 – F90.1)
• attention-deficit/hyperactivity disorder combined presentation (ADHD/C) (314.01 – F90.2)
• ADHD other specified and unspecified ADHD (314.01 – F90.8).
2 Evaluate child (as appropriate for age/developmental status): Discuss peer/family relationship/school/behavior concerns (esp any anxiety and depression, abuse, trauma, bullying); encourage self-assessment of fxn/performance, perform PE/neuro exam, observe behavior. For adolescents: Use validated self-report instrument of ADHD and coexisting conditions.
• For children 4-5 yo not yet in school, validated rating scales (eg, Conners or ADHD Rating Scale IV) may be helpful in the dx eval.
• Specific behaviors in the DSM-5 criteria for ADHD are the same for all children younger than 18 yo and are only minimally different from the DSM-IV.
• If the ADHD Rating Scale-5 or the ADHD Rating Scale-IV Preschool Version isn’t available, any other DSM-based scale can be used.
• Neuropsychological testing hasn’t been found to often improve diagnostic accuracy, but may clarify the child or adolescent’s learning strengths and weaknesses.
3 Obtain info from family (parent, guardian, other frequent caregivers): Ascertain concerns/HPI, obtain FHx including trauma and acute stressors + PMH/psychosocial history/ROS, apply validated ADHD instrument, consider concomitant issues, ascertain general fxn.
4 Gather info from school (and important community informants): Ascertain concerns and how pt functions in academic, work, and social interactions, apply validated ADHD instrument, consider comorid conditions, review academic/administrative reports.
• For adolescents (ages 12 to 18 yo): Obtain info from at least 2 teachers or other sources, such as coaches, school guidance counselors, or leaders of community activities in which the adolescent participates. Eval success depends on adolescent consent/participation in the eval.
5 For example, anxiety, depressive, oppositional defiant, and conduct disorders, substance use.
6 For example, learning and language disorders, autism spectrum disorders.
7 For example, tics, sleep apnea.
8 For example, suicidal thoughts/acts or other behaviors w/ potential to severely injure child/adolescent or others, such as severe temper outbursts or child abuse.
9 [DSM-5: only 5 (rather than 6) criteria needed for pts ≥17 yo | Epocrates note].
10 DSM-5: <12 yo for sx onset. Unless they previously received a diagnosis, to meet DSM-5 criteria for ADHD, adolescents must have some reported or documented manifestations of inattention or hyperactivity/impulsivity before age 12. -
Preschool children (4-5 yo) Behavioral tx is 1st line: evidence-based, delivered by parent and/or teacher (parent training in behavior management and/or behavioral classroom interventions) [A/S] If behavioral tx fails/unavailable and mod-severe1 functional disturbance continues, methylphenidate2-4 may be used [B/R]; weigh risks of starting med @ early age vs harms of delayed tx [B/S] - Start @ low dose5 and titrate q3-7days5 to max effect/min side effects [B/S]
- During 1st mo, titration may be done w/ weekly or biweekly F/U
- Alert parents that changing med/dose may be necessary for optimal med mgmt, can take a few mo for optimal success, and that med efficacy needs monitoring @ regular intervals
- Schedule face-to-face F/U by 4th wk of medication to review response and monitor for ADR, pulse, BP, and wt
- F/U monthly until consistent, optimal response observed, and q3mo thereafter during 1st yr of tx
- Subsequent visits depend on response but should occur at least 2 times/yr until clear that target goals are progressing and sx stabilized, then periodically, as determined by family and treating clinician
- Monitor improvement in core sx6/target goals in objective way whenever possible w/ 1 of the DSM-5-based ADHD rating scales
- If sx improve after several years: Consider initiating a trial off of the med to determine if still needed
- If sx do not improve: Re-eval to confirm dx, assess for coexisting condition, and provide education to improve adherence; reconsider tx plan: Change med/dose or add med approved for adjuvant tx, and/or change behavioral tx
Address urgent conditions (eg, acts/behaviors w/ potential to injure the child or others, such as severe temper outbursts or child abuse) immediately w/ services capable of handling crisis situations Manage ADHD as chronic condition [B/S] - Children w/ ADHD have special healthcare needs
- Mgmt should follow principles of chronic care/medical home model [B/S]
Certain non-med tx aren’t recommended for treating ADHD due to lack of evidence and/or findings that show little or no benefit: - Mindfulness
- Cognitive training
- Diet modification
- EEG biofeedback
- Supportive counseling
- Cannabidiol oil
- eTNS
Drug Links | Methylphenidate Footnotes 1 Mod-severe dysfxn = sx for ≥9 mo, dysfxn @ home and another setting (eg, daycare); dysfxn not improved w/ PTBM. Evidence-based parent training in behavior management (PTBM) training typically begins with 7-12 wkly group or individual sessions w/ a trained or certified therapist. Although PTBM treatments differ, the primary focus is on helping parents improve strategies for rewarding/motivating child to reduce ADHD behavioral difficulties.
2 Methylphenidate use in preschool-aged children remains off-label, though there is moderate evidence that it’s safe and efficacious. Preschool-aged children may experience ↑mood lability and dysphoria w/ stimulant meds. None of the nonstimulants have FDA approval for use in preschool children.
3 Although cardiac illness is rare, clinicians should obtain careful hx of cardiac sx in child/adolescent + cardiac FHx incl. sudden death, CV sx, Wolff-Parkinson-White syndrome, hypertrophic cardiomyopathy, and long QT syndrome. If any of these risk factors present, obtain further eval w/ ECG and consult w/ pediatric cardiologist before initiating ADHD stimulant med tx.
4 Most common stimulant ADRs: ↓appetite, abdo pain, headache, sleep disturbance. Preschool-aged children may experience ↑mood lability and dysphoria.
5 Young children (ages 4-5 yo) may metabolize stimulants slower than older children; starting dose should be lower and increased in smaller increments.
6 Core sx can be monitored w/ rating scales that use the DSM-5 criteria for ADHD. Changes in the 18 core sx are essentially unchanged from DSM-IV criteria so DSM-IV–based rating scales can be used if DSM-5 rating scales aren’t readily available.
Elementary school children (6-11 yo) Prescribe FDA-approved ADHD med [A/S], along w/ parent training in behavior management (PTBM) and/or behavioral classroom interventions (preferably both) [A/S] - Evidence strongest for stimulants,1,2 followed by atomoxetine,3 guanfacine ER,4 and clonidine ER4 [A/S]
- Start stimulant at low dose and titrate q3-7days to max effect/min side effects [B/S]
- During 1st mo, titration may be done w/ weekly or biweekly phone call F/U
- Alert parents that changing med/dose may be necessary for optimal med mgmt, can take a few mo for optimal success, and that med efficacy needs monitoring @ regular intervals
- Schedule face-to-face F/U by 4th wk of medication to review response and monitor for ADR, pulse, BP, and wt
- F/U monthly until consistent optimal response observed, and q3mo thereafter during 1st yr of tx
- Subsequent visits depend on response but should occur at least 2 times/yr until clear that target goals are progressing and sx stabilized, then periodically, as determined by family and treating clinician
- Monitor improvement in core sx5/target goals in objective way whenever possible w/ 1 of the DSM-5-based ADHD rating scales
- If sx improve after several yrs: Consider initiating a trial off of the med to determine if still needed
- If sx do not improve: Re-eval to confirm dx, assess for coexisting condition, and provide education to improve adherence; reconsider tx plan: Change med/dose6 or add med approved for adjuvant tx,7 and/or change behavioral tx
Behavioral tx: - Support evidence-based parent/teacher-administered behavioral tx [A/S]
- Educational interventions and individualized instructional supports, incl school environment, class/instructional placements, and behavioral supports must be part of any tx plan and often include an Individualized Education Plan (IEP) or a rehab plan (504 plan)
Address urgent conditions (eg, suicidality, acts/behaviors w/ potential to injure the child or others, such as severe temper outbursts or child abuse) immediately w/ services capable of handling crisis situations; substance use disorders require immediate attention and may precede/coincide w/ ADHD tx Manage ADHD as chronic condition [B/S] - Children w/ ADHD have special healthcare needs
- Mgmt should follow principles of chronic care/medical home model [B/S]
Certain non-med tx aren’t recommended for treating ADHD due to lack of evidence and/or findings that show little or no benefit: - Mindfulness
- Cognitive training
- Diet modification
- EEG biofeedback
- Supportive counseling
- Cannabidiol oil
- eTNS
Drug Links | Stimulants - Methylphenidate (long-acting) Drug Links | Stimulants - Methylphenidate (short-acting) Drug Links | Stimulants - Amphetamine (long-acting) Drug Links | Stimulants - Amphetamine (short-acting) Drug Links | Nonstimulants Footnotes 1 Although cardiac illness is rare, clinicians should obtain careful hx of cardiac sx in child/adolescent + cardiac FHx incl sudden death, CV sx, Wolff-Parkinson-White syndrome, hypertrophic cardiomyopathy, and long QT syndrome. If any of these risk factors present, obtain further eval w/ ECG and consider consult w/ pediatric cardiologist before initiating ADHD stimulant med tx.
Educate parents that although meds can facilitate schoolwork production, they haven’t been shown to be effective for learning disabilities. A child who continues to experience academic underachievement after attaining ADHD behavioral sx control should be assessed for a coexisting condition (eg, learning/language disabilities, other mental health disorders, or other psychosocial stressors).
2 Stimulant ADRs:↓ appetite, abdo pain, HA, sleep disturbance. ↓ growth velocity seen esp w/ higher, more consistently administered doses; effects diminished by 3rd yr of tx w/ no compensatory rebound observed; diminished growth ≈1-2 cm. Hallucinations/other psychotic sx uncommon; sudden cardiac death extremely rare.
3 Atomoxetine ADRs: initial somnolence and GI sx (esp, if rapid dose escalation), ↓ appetite; ↑ suicidal thoughts (black box warning) less common, and hepatitis. Also linked to growth delays compared to expected trajectories in first 1-2y of tx, w/ return to expected measurements after 2-3y of tx on average.
4 Guanfacine ER/clonidine ER ADRs: somnolence, dry mouth, dizziness, irritability, HA, bradycardia, hypotension, and abdo pain. Taper off vs sudden discontinuation d/t rebound hypertension risk.
5 Core sx can be monitored w/ rating scales that use the DSM-5 criteria for ADHD. Changes in the 18 core sx are essentially unchanged from DSM-IV criteria so DSM-IV–based rating scales can be used if DSM-5 rating scales aren’t readily available.
6 If max dose of stimulant reached and less than satisfactory results achieved or intolerable ADRs occur before adequate efficacy w/ a med from 1 stimulant group (methylphenidate or amphetamine), may use a med from the other stimulant group w/ similar titration plan. At least half of children whose sx fail to respond to 1 stimulant med may have a positive response to alternative med.
7 Guanfacine ER or clonidine ER may be added as adjunctive tx in children who partially respond to a stimulant.
Prescribe FDA-approved ADHD med w/ pt consent [A/S] and evidence-based training interventions and/or behavioral tx [A/S], preferably both - Start stimulant1,2 at low dose and titrate q3-7days to max effect/min side effects [B/S]
- During 1st mo, titration may be done w/ weekly or biweekly phone call F/U
- Alert parents that changing med/dose may be necessary for optimal med mgmt, can take a few mo for optimal success, and that med efficacy needs monitoring @ regular intervals
- Schedule face-to-face F/U by 4th wk of medication to review response and monitor for ADR, pulse, BP, and wt
- F/U monthly until consistent, optimal response observed, and q3mo thereafter during 1st yr of tx
- Subsequent visits depend on response but should occur at least 2 times/yr until clear that target goals are progressing and sx stabilized, then periodically, as determined by family and treating clinician
- Monitor improvement in core sx3/target goals in objective way whenever possible w/ 1 of the DSM-5-based ADHD rating scales
- If sx improve after several yrs: Consider initiating a trial off of the med to determine if still needed
- If sx do not improve: Re-eval to confirm dx, assess for coexisting condition, and provide education to improve adherence; reconsider tx plan: Change med/dose,4 or add med approved for adjuvant tx,5 approved for adjuvant tx,5 and/or change behavioral tx
Ensure medication coverage for sx control for times when adolescent may exhibit risky behaviors such as driving or spending unsupervised time w/ friends: - Consider longer-acting meds or late-afternoon admin of nonstimulant meds or short-acting meds
Assess pts for substance abuse sx; address urgent conditions (eg, suicidality, acts/behaviors w/ potential to injure the adolescent or others, such as severe temper outbursts or child abuse) immediately w/ services capable of handling crisis situations; substance use disorders require immediate attention and may precede/coincide w/ ADHD tx - Diversion of ADHD meds is a concern—whether by adolescents or individuals w/ close contact—and warrants monitoring sx and refill requests
- Consider prescribing meds w/ no abuse potential6 or stimulants w/ less abuse potential7
- Note: Short-acting, mixed amphetamine salts are the most commonly misused or diverted ADHD med
Manage ADHD as chronic condition [B/S] - Adolescents w/ ADHD have special healthcare needs
- Mgmt should follow principles of chronic care/medical home model [B/S]
Certain non-med tx aren’t recommended for treating ADHD due to lack of evidence and/or findings that show little or no benefit: - Mindfulness
- Cognitive training
- Diet modification
- EEG biofeedback
- Supportive counseling
- Cannabidiol oil
- eTNS
Drug Links | Stimulants - Methylphenidate (long-acting) Drug Links | Stimulants - Methylphenidate (short-acting) Drug Links | Stimulants - Amphetamine (long-acting) Drug Links | Stimulants - Amphetamine (short-acting) Drug Links | Nonstimulants Footnotes 1 Although cardiac illness is rare, clinicians should obtain careful hx of cardiac sx in child/adolescent + cardiac FHx incl. sudden death, CV sx, Wolff-Parkinson-White syndrome, hypertrophic cardiomyopathy, and long QT syndrome. If any of these risk factors present, obtain further eval w/ ECG and consider consult w/ pediatric cardiologist before initiating ADHD stimulant med tx.
Educate parents that although meds can facilitate schoolwork production, they haven’t shown to be effective for learning disabilities. A child who continues to experience academic underachievement after attaining ADHD behavioral sx control should be assessed for a coexisting condition (eg, learning/language disabilities, other mental health disorders, or other psychosocial stressors).
2 Stimulant ADRs: ↓appetite, abdo pain, headache, sleep disturbance. ↓growth velocity seen esp w/ higher, more consistently administered doses; effects diminished by 3rd yr of tx w/ no compensatory rebound observed; diminished growth ≈1-2 cm. Hallucinations/other psychotic sx uncommon; sudden cardiac death extremely rare.
3 Core sx can be monitored w/ rating scales that use the DSM-5 criteria for ADHD. Changes in the 18 core sx are essentially unchanged from DSM-IV criteria so DSM-IV–based rating scales can be used if DSM-5 rating scales aren’t readily available.
4 If max dose of stimulant reached and less than satisfactory results achieved or intolerable ADRs occur before adequate efficacy w/ a med from 1 stimulant group (methylphenidate or amphetamine), may use a med from the other stimulant group w/ similar titration plan. At least half of adolescents whose sx fail to respond to 1 stimulant med may have a positive response to alternative med.
5 Guanfacine ER or clonidine ER may be added as adjunctive tx in adolescents who partially respond to a stimulant.
6 ADHD meds w/ no abuse potential (nonstimulants): atomoxetine, guanfacine ER, clonidine ER.
7 Stimulants w/ less abuse potential: lisdexamfetamine, dermal methylphenidate, or OROS methylphenidate.
Does not meet DSM ADHD criteria No medication indicated, continue enhanced surveillance - Educate family and child/adolescent (incl trigger identification/elimination), behavior mgmt options, strategies for improving school performance/behavior
- Encourage parents to complete parent training in behavior management (PTBM),1 the recommended primary intervention children w/ ADHD-like behaviors whose diagnosis is not yet verified
Footnotes 1 Evidence-based parent training in behavior management (PTBM) training typically begins with 7-12 wkly group or individual sessions w/ a trained or certified therapist. Although PTBM treatments differ, the primary focus is on helping parents improve the strategies for rewarding/motivating child to reduce ADHD behavioral difficulties.
|